
The U.S. Government Is a Health Insurance Company With a Small Standing Army
Healthcare isn't starved for funds
A truly dimwit take on the left is to claim we don’t have universal health care because we spend too much money on warfare, or Trump’s White House ballroom, or some other political project they don’t like. Of course, the military is the biggest target. Those B-2 bombers could just eliminate my copay for Viagra, right?
The problem is that the slogan does not survive contact with arithmetic.
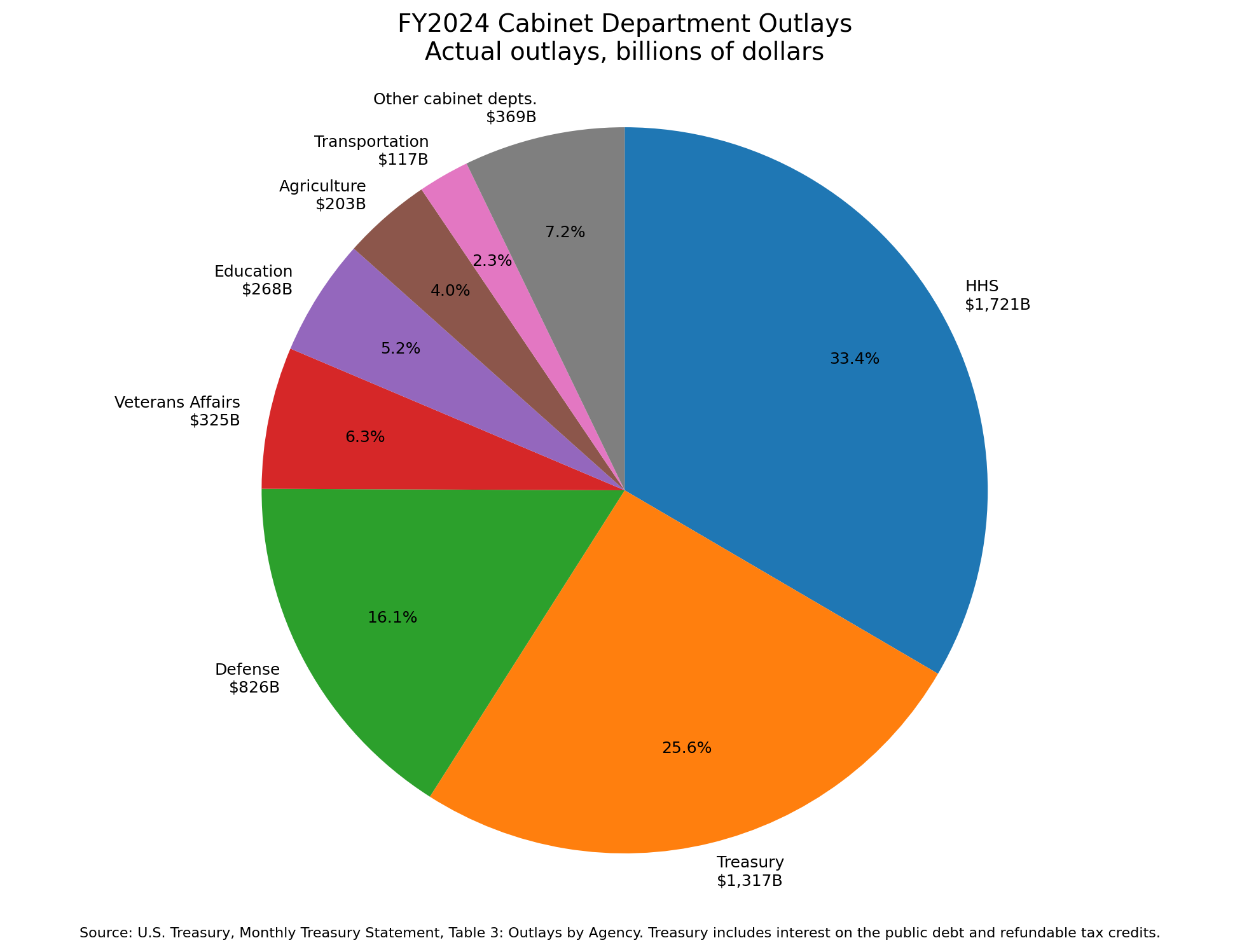
In fiscal year 2024, the Department of Health and Human Services spent $1.721 trillion. The Department of Defense spent $826.3 billion in agency outlays. HHS was not a minor social program hiding in the shadow of the Pentagon. It was more than twice the size of the Defense Department by that measure. The HHS total was driven overwhelmingly by the Centers for Medicare and Medicaid Services, which accounted for about $1.5 trillion of HHS spending. Even if one uses SIPRI’s broader international definition of U.S. military expenditure, which puts American military spending at $997 billion in 2024, the basic point does not change. The federal government is not a military machine that occasionally pays for healthcare. It is a gigantic health insurance company with a very expensive military attached.
Zoom out beyond the federal budget, to the economy as a whole, and the picture becomes even harder to square with the usual story. Total U.S. health spending reached $5.3 trillion in 2024, or 18.0 percent of GDP. Medicare alone accounted for $1.118 trillion. Medicaid accounted for $931.7 billion. Private health insurance accounted for another $1.645 trillion. That is 18 percent of GDP, taken from taxes, payroll, and premiums, routed through numerous third parties, and handed to various entities to provide healthcare. Meanwhile, the military takes roughly 3.4 percent of our GDP.
This distinction matters because bad arithmetic leads to bad politics. It is easy to say patients would be better off if we simply took money from the Pentagon and dropped it into HHS. But I do not see how anyone who has spent time inside American healthcare can believe that with a straight face.
The system doesn’t lack money.
The money just flows through a machine that is exquisitely designed to reward everything except simple, affordable, accountable care.
To say this is not to deny the reality patients experience. Medicaid patients routinely struggle to get timely specialty care, even for procedures that, in a cash market, can cost only a few thousand dollars. Even privately insured patients often feel like they’re getting second-rate care. But that is exactly the point. American healthcare can be lavishly funded at the institutional level and brutal at the patient level. A hospital can build a tower, expand a billing department, acquire physician practices, employ armies of coders, and still leave a working mother unable to get an affordable appointment for her child.
The deeper problem is that American healthcare is not a normal market. It is a centrally planned, inefficient behemoth. And dumping more funding into a distorted system does not necessarily buy more care. It can buy more distortion. It can inflate hospital prices, reward consolidation, expand compliance departments, deepen dependence on third-party payment, and give incumbents another reason not to change. A dollar routed through a badly designed payment machine does not reach the patient.
The great irony is that many of the people who complain most loudly about healthcare costs keep asking for more of the thing that created them: more government. Then, when prices rise and access remains miserable, they conclude that the answer must be still more money.
The Pentagon wastes money. Of course it does. Every large bureaucracy wastes money, and defense procurement is not exactly a monastery of thrift. But the idea that American healthcare is poor because defense is rich is a myth. It allows us to avoid the harder question: why does a country spending $5.3 trillion on healthcare still make ordinary patients feel like they are begging for access to a system they already paid for?
That question is much more uncomfortable than “bombs versus bandages,” because it points back at the machinery of healthcare itself, and how government intervention created this mess.
Taking the entire defense budget and dumping it into HHS would not produce a golden age of patient care. It would make an already enormous department even larger. Unless the incentives changed, the new money would flow where the old money already flows: toward hospitals with market power, administrative infrastructure, billing sophistication, compliance machinery, and political leverage.
Healthcare scarcity in America is not caused primarily by the Pentagon. It is caused by a payment architecture that hides prices, suppresses tradeoffs, rewards rent extraction, and protects incumbents from competition. We do not need to pretend the military is cheap to see this. We only need to stop pretending healthcare is poor.
"The money just flows through a machine that is exquisitely designed to reward everything except simple, affordable, accountable care."
That is true as far as it goes, but some of the rewards (endovascular treatment of ischemia, cancer cures unimaginable 10 years ago, simple cataract removal, etc x 20) are both costly and desirable. And yes, of course, with third party payment either RVU based or episode based, there is fluff, profiteering, and bias toward treatment.
What is costly and not at all desirable is the gigantic administrative superstructure that has grown and metastasized in the last ten years. The pool of money provided by governments and employers for the care of the sick is now feeding many hungry stomachs that have nothing to do with the sick, but rather serve to optimize the share of that pool going to nonclinical and nonproductive work.