
Medicare’s “Low Administrative Costs” Are an Accounting Trick
Is the government really cheaper than the private sector?
One of the most durable claims in American healthcare politics is that Medicare is administratively efficient because its official overhead is low.
The argument usually arrives as a conversation-ender, often with a snide, “Well, Medicare only spends 6% on administration, therefore it must be more efficient.”
Of course, anyone who has watched the government do much of anything knows that efficiency is not exactly its strong suit. Even the things the government is supposedly good at, like war, tax collection, and national parks, tend to be run with layers of process and waste. How much have we burned through on failed fighter jet plans?
Then comes the second move: private insurance wastes money on marketing, administration, and, of course, that evil term: profits.
That sounds persuasive until you ask the most basic economic question: for whom is Medicare actually efficient?
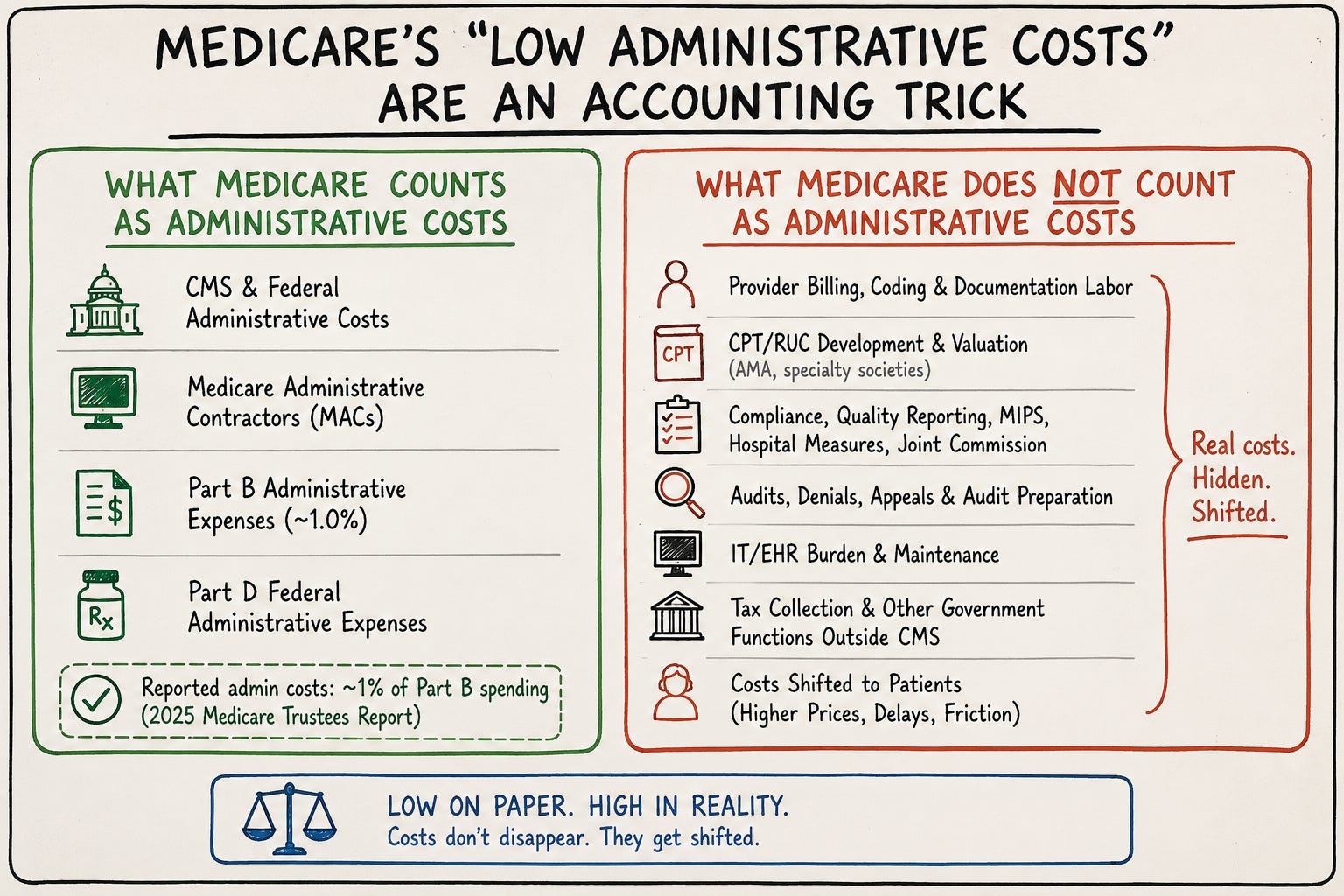
Medicare does not have magically low administrative costs. It has narrowly measured administrative costs, unusually expensive beneficiaries, and a large hidden bureaucracy that is offloaded to entities outside of CMS. The official number may be low on the Medicare ledger, but that does not mean the administrative burden has disappeared.
Ask any physician who has dropped Medicare. They will often tell you their administrative costs dropped dramatically. No more conditions of participation, quality metric reporting, Medicare audits, Stark law headaches… the list goes on.
This is the part physicians understand instinctively because we live inside the machinery. Medicare is not a frictionless payment system. It is a world of CPT and ICD-10 codes. CMS did not single-handedly create every bad EHR, but federal policy helped make inefficient EHRs unavoidable, and the result is that clinicians now spend staggering amounts of time feeding the record rather than caring for patients.
The official Medicare numbers are not fake. They are simply incomplete for the political work they are being asked to do. The 2026 Medicare Trustees Report estimated that Medicare covered 69.3 million people in 2025 and spent about $1.21 trillion. The same report lists relatively small explicit administrative expense lines, including about $5.9 billion in Part B administrative expenses, equal to 1.0 percent of Part B expenditures, and about $0.5 billion in federal administrative expenses for Part D.
The first trick is the denominator. Medicare beneficiaries are older and sicker than the average privately insured person, so Medicare spends far more in medical claims per enrollee. When administrative costs are presented as a percentage of total spending, a program that pays very large medical bills will naturally look administratively leaner.
CMS national health expenditure data show that, in 2020, per-person personal healthcare spending for adults age 65 and older was $22,356, more than five times spending for children and nearly two and a half times spending for working-age adults. Older adults were about 17 percent of the population but accounted for roughly 37 percent of personal healthcare spending.
Imagine two insurers spend the same amount administering a patient. One patient generates $5,000 in annual claims. The other generates $25,000. The same administrative cost will look five times smaller as a percentage of claims in the second case. Nothing about that proves the second insurer is more efficient. It proves the patient is more expensive.
The second trick is the accounting boundary. Medicare’s official administrative cost includes payments to Medicare Administrative Contractors, the private contractors that process claims and perform much of the operational work of traditional Medicare. But they offload a lot more.
Medicare offloads collection of premiums to other branches of the government. Where a private insurance company has to spend money on premium collection, Medicare relies on the IRS to collect the taxes to pay for its services. No cost to CMS there.
Medicare also offloads the work of describing and valuing the billing units for physicians. Much of this happens through the CPT and RUC machinery, maintained outside CMS by the AMA and specialty societies. There are millions of dollars worth of time from physicians and staff for which Medicare never pays. Then, of course, physicians pay for coding courses. Practices pay coders, who also attend those coding courses. Staff spend hours learning how to navigate CPT codes and documentation rules. None of that shows up as CMS administrative overhead. Meanwhile, private insurance companies are responsible for negotiating their own distinct contracts with numerous provider groups.
Then, of course, there are the quality metrics.
One study in JAMA Health Forum estimated that physician practices spent an average of $12,811 per physician and more than 200 hours per physician to participate in MIPS in 2019. The authors estimated that physicians themselves accounted for more than half of the financial cost, because physician time was absorbed by compliance rather than patient care. Another study in Health Affairs estimated that U.S. physician practices spent an average of 785 hours per physician per year on quality-measure reporting, at a total annual cost of more than $15.4 billion. A study of hospital quality reporting in JAMA estimated that reporting 162 quality metrics required more than 108,000 staff-hours and about $5 million in annual personnel costs at one major academic medical center.
These are not abstractions. These are hours and dollars that could have been spent on actual patient care. And this is exactly the sort of cost that disappears when we pretend Medicare’s administrative cost is whatever CMS spends directly to run the program.
The third trick is cost-shifting. Government programs are very good at making costs vanish from one ledger by imposing them on another. A regulation can look cheap to the agency that issued it if the work of compliance is performed by someone else.
This is one of the underappreciated ways bureaucracy drives consolidation. Large hospital systems can absorb the administrative burden. Small independent practices cannot. When policy makes fixed administrative costs unavoidable, it favors scale. Then policymakers express surprise when physicians sell their practices to hospitals, prices rise, and patients lose access to independent doctors.
The data point in that story is no longer subtle. GAO reported that at least 47 percent of physicians were consolidated with hospital systems in 2024, up from less than 30 percent in 2012. GAO also noted that physician-hospital consolidation can increase Medicare spending when services move into more expensive hospital-based settings.
None of this means private insurance is innocent. Private insurance has its own enormous administrative machinery. Some of it is duplicative. Much of it is maddening. Every physician in America has lost hours of life to insurer portals and peer-to-peer calls that seem designed less to improve care than to exhaust the person trying to provide it.
But we should be careful with the word “waste.” In ordinary markets, advertising, profit, sales, customer service, contracting, and risk management are not automatically waste. We do not say the iPhone is inefficient because Apple advertises and earns a profit. Those activities may be costly, but in a functioning market they are part of how firms compete. If Apple could sell as many iPhones with half of its advertising budget, it would cut that cost in an instant. The problem in healthcare is not that private insurers have administrative costs. The problem is that our third-party payment system hides prices, insulates patients from tradeoffs, and forces clinicians to negotiate with payers rather than directly with the people receiving care.
Private insurance deserves plenty of criticism. Yet private insurance, if the market is working as it should, disciplines itself. Whichever insurer can keep administrative costs the lowest should outcompete the others by providing quality coverage at lower prices. There are plenty of reasons the market is distorted and not working as efficiently as it should, but the underlying principle is the same. There is no comparable discipline on Medicare. There is no true competition with other forms of insurance keeping the system honest.
Medicare does not become efficient merely because it avoids some private-sector costs while imposing a different set of public-sector costs. Just because Medicare lacks a marketing department does not automatically mean it is efficient.
There is also a deeper point that rarely appears in these debates: low administrative spending is not automatically good. A trillion-dollar public program needs oversight. If it does not spend enough on administration up front, it will spend more later through improper payments, blunt audits, or after-the-fact enforcement. CMS reported FY2025 improper payment estimates of $28.83 billion for Medicare fee-for-service, $23.67 billion for Medicare Advantage, and $4.23 billion for Part D. Maybe a little more administration would be a good thing here.
This is the central error in the Medicare expansion argument. It takes a narrow accounting ratio and treats it as a complete economic fact.
The physician’s unpaid evening documentation, the quality department at the hospital, and the compliance officers are all costs. The patient waiting six months because independent practices in the area stopped taking new Medicare patients is a cost.
Healthcare policy should begin with acknowledging scarcity, tradeoffs, and incentives. That means asking not only how much Medicare spends on its own administration, but how much administrative work Medicare causes other people to perform.
The point is not that Medicare is all bad. Medicare pays for a tremendous amount of necessary care. Every hospital in America depends on it. Millions of elderly and disabled patients would be in deep trouble without it. The point is that we should stop using a narrow overhead statistic as if it settles the question of efficiency.
It does not.
Administrative costs do not disappear simply because the government does not count them.