
Inefficiency in Medicine
How the Keyboard Ate Technology
Compared to our relatively recent ancestors, humans today are much more productive with their time. I mean that literally. Imagine the amount of food or clothing a human could produce with their labor 100 years ago compared to now. Then look at advanced manufacturing, robotics, and now AI. The statistics show this. Just in the last thirty years, private nonfarm business productivity rose 78 percent. That means for every hour of work, the average American produces 78% more stuff now than they did in the 1990s.
Except in healthcare.
There, the statistics are more dire: growth in labor productivity of about 1.5% from 1993 to 2022.
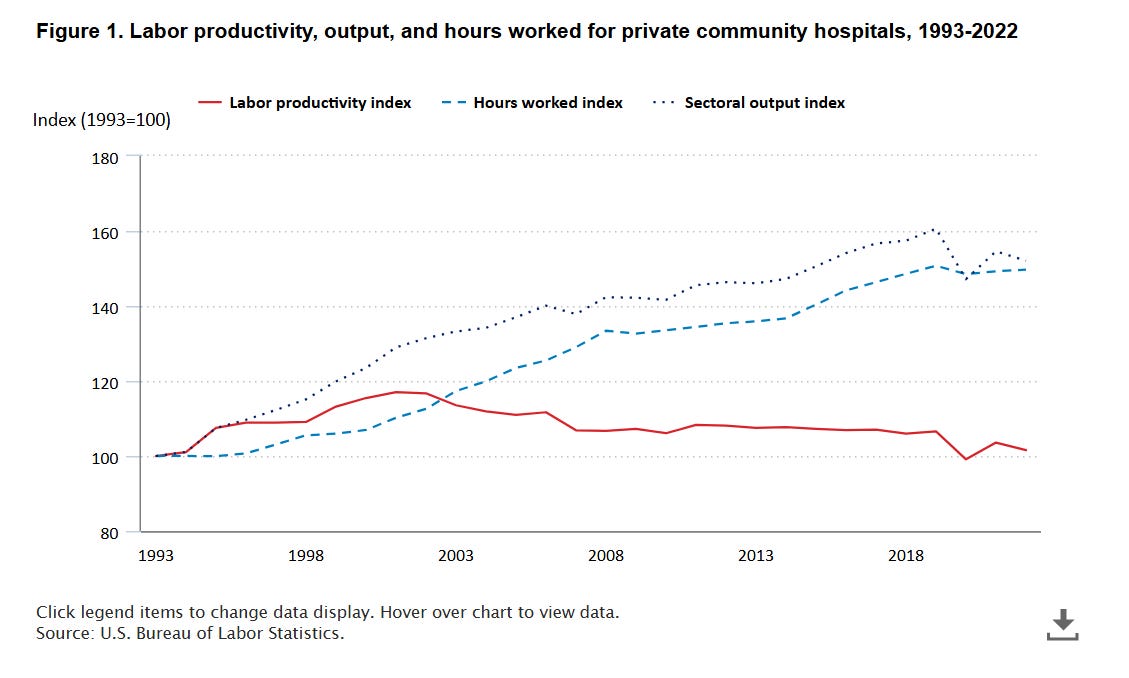
So while the average American worker is nearly twice as productive, the average hour of hospital labor is only about 1.5 percent more productive.
That is an astonishing fact.
This is despite massive improvements in healthcare technology, including imaging, laboratory medicine, devices, and pharmaceuticals. Many surgical techniques have been refined with smaller incisions and minimally invasive tools to cut down on operative time and hospital stays.
What’s even more astounding is that healthcare labor productivity has been flat during the information technology revolution. In 1993, patient charts were on paper. Lab results had to be printed out and physically placed in the chart, visible only to the person who possessed the physical copy. X-ray, CT, and MRI results were printed on plastic films that had to be hung on light boxes in the office. There was almost no portability of records.
Now we have digital records, lab results, and imaging that are far more portable than anything we had in the age of paper. Yet we are no more productive than we were then.
In a normal market, thirty years of flat productivity would signal a dying industry. It would mean that competitors were coming. Capital would flee. Customers would demand better. New entrants would find ways to do the same job cheaper, faster, or more conveniently. But in American healthcare, flat productivity does not signal failure in the usual market sense. It signals a protected, heavily regulated, third-party-paid system functioning more or less as designed.
Hospitals have not been forced to become more productive because the economic system around them does not reward productivity in the way normal markets do. The patient is not really the customer. Payment is filtered through Medicare rules, Medicaid supplemental schemes, and opaque cross-subsidies that no ordinary human being could possibly understand. In such a system, the path to survival is not necessarily to deliver more care at lower cost. It is to become better at navigating the payment maze.
This is the productivity paradox in American hospitals. We have extraordinary medical technology, highly trained clinicians, and an economy that has learned how to make nearly everything else more efficient. Yet the hospital, the central institution of American healthcare, appears to have resisted the productivity revolution.
The usual explanation is Baumol’s cost disease. Medicine, we are told, is a high-touch service industry. You cannot automate compassion. Patients are older, sicker, more complex, and more medically fragile than they were thirty years ago. Therefore, the argument goes, we should not expect hospitals to achieve productivity gains comparable to manufacturing, retail, logistics, or software.
This is the kind of half-truth that protects an inefficient system from scrutiny.
Yes, healing is different from making widgets. But anyone who has practiced medicine over the last few decades knows that clinical work itself has not been frozen in amber. We are not practicing 1993 medicine. MRI did not replace the neurological exam, but it radically compressed diagnostic uncertainty. Countless other technologies have improved the speed and precision of care. Much of what once required exploratory surgery, serial exams, prolonged hospitalization, or educated guesswork can now be seen, measured, and treated with tools that would have seemed miraculous to physicians a generation ago.
Ask any practicing physician where the missing productivity went, and he will not give you a lecture on Baumol. He will point to the electronic health record and the endless parade of mandatory clicks that seem to multiply faster than any real clinical need.
The Annals of Internal Medicine time-motion study on ambulatory physicians found that for every hour physicians spent in direct clinical face time with patients, they spent nearly two additional hours on EHR and desk work during the clinic day. Outside office hours, they spent another one to two hours each night doing additional clerical and computer work.
This is where the productivity gains went. The time saved by better technology was consumed by more administrative work and data entry. We invented tools that should have made the physician more productive, then wrapped those tools in billing rules and compliance rituals until they became a tax on clinical judgment.
The EHR was sold as a tool for better information. But the EHR did not emerge into a functioning market for medical care. It emerged into a reimbursement bureaucracy. Medicare’s “meaningful use” program required physicians using certified EHR technology to capture, exchange, and report specific clinical data and quality measures, beginning in 2011. That transformed the chart from a clinical record into a billing document that happened to contain some medical information.
That distinction matters. A clinical note is supposed to communicate what is wrong with the patient and what we are going to do about it. A billing note is a different product. We pretend they are the same document because the fiction is convenient for everyone except the people actually taking care of patients.
In many clinics, expensive clinical labor is now deployed to feed the chart before the visit even begins. Some of this work is clinically useful. Much of it is defensive. The purpose is not always to understand the patient better. Often it is to make the chart billable, auditable, and administratively complete. You’ve probably experienced this every time you go to a doctor’s visit and are asked to fill out a stack of paperwork.
The hospital labor force reflects the same problem. Paragon notes that hospital employees per bed rose from 4.56 in 2000 to 6.32 in 2023, a 39 percent increase. To be fair, some of that may reflect more complex inpatient care as simpler services move outpatient. But it also raises the obvious question: how many of those additional workers are making patients better, and how many are helping the institution survive the administrative complexity we have built around care?
The defenders of the status quo will object that healthcare is complicated. They are right. But they often draw exactly the wrong conclusion from that fact.
Because healthcare is complicated, we should be more humble about centralized control, not more ambitious. Complexity is an argument for better feedback, not an argument for more bureaucracy. It is an argument for prices that patients can see, contracts that physicians can understand, and institutions that must compete on value rather than market power and coding sophistication. That’s how efficiency is rewarded.
In the rest of the economy, software tends to reduce friction. It lets a small business manage payroll, inventory, communication, accounting, advertising, and sales with tools that would once have required entire departments. In healthcare, software often does the opposite. It creates new work, new alerts, new compliance pathways, new reporting obligations, and new opportunities for denial.
That is the difference between technology disciplined by customers and technology disciplined by regulators and payers.
This is why the “Baumol’s cost disease” story is so incomplete. It treats hospital productivity stagnation as if it were an unavoidable feature of human care. But the lived reality of medicine suggests something more specific and more damning. We did not fail to invent productivity-enhancing tools. We invented many of them. Then we embedded them in a financing system that converted clinical time into administrative output.
The MRI made diagnosis faster. The EHR made documenting the diagnosis slower.
Because this is ultimately a policy choice, we should stop pretending that the solution is another layer of policy complexity. The answer begins with the recognition that productivity in medicine will not improve until the people delivering care are rewarded for delivering care, rather than for feeding the documentation machine.
American hospitals do not have flat productivity because healing is immune to improvement. They have flat productivity because we have built a financing and regulatory structure that protects inefficiency and rewards administrative sophistication at the expense of true efficiency. Until that changes, technology will keep making medicine more expensive rather than more productive.
I am thankful to you for sharing your insights in this article. It reminded me that healthcare is a payor-driven system: employers and employees entrust their healthcare dollars to third-party payors and taxpayers entrust tax dollars to CMS to cover healthcare services for their beneficiaries. Both systems are designed in such a way that they pay more for more services. In that regard it is in the controlling entities’ best interests to limit provider productivity and limit access for their beneficiaries. I find it alarming that many of their actions do not take into account the health outcomes of the very same patients that “gave” them their money to begin with. By their actions, payors provide evidence that the outcomes that matter most are retaining the funds entrusted to them to manage care.