
Doctors Are Not Crashing Jumbo Jets
Medical Errors Are Not a Leading Cause of Death
Imagine an elderly patient who had bleeding in her brain. She had fallen, hit her head, and now had a little spot of blood between the brain and the skull. She had been placed on a blood thinner by her primary care doctor because of an abnormal heart rhythm. People with this abnormality, called atrial fibrillation, or a-fib, are placed on a blood thinner because they are prone to blood clots that can cause strokes. The blood thinner helps prevent clots and lowers the chance of stroke, which is why modern atrial fibrillation guidelines generally recommend anticoagulation for patients whose stroke risk is high enough, while also forcing doctors to weigh the competing risk of bleeding.
Now, of course, the blood thinner was causing a problem. She had blood in her head, and if it continued to bleed, it could become life-threatening. So doctors had to stop her blood thinner. When the bleeding got a bit bigger on a repeat CT scan, the team reversed the blood thinner with a medication that restored her blood’s natural ability to clot. The bleeding in her head stopped getting bigger, and she was stable.
Two days later she suffered a massive stroke and died.
Was it an error to reverse her blood-thinning medication? We can never know the counterfactual. Had she continued her blood thinner, there is a chance the intracranial bleeding would have stopped anyway. Maybe she avoids having the stroke and lives another few years. Maybe the hemorrhage continues and she dies after undergoing an unsuccessful operation to save her life. We can never know.
But this is exactly the kind of case that becomes dangerous when judged backward by a reviewer who already knows the outcome. If she dies of the expanding brain bleed, the reviewer can ask why anyone continued anticoagulation in an elderly fall patient with blood in her head. If she dies of the stroke after anticoagulation is reversed, the reviewer can ask why anyone stopped the medicine that was protecting her from embolic stroke. The same clinical tradeoff can be condemned from opposite directions depending entirely on which bad outcome occurred.
You have probably heard the viral claim that doctors’ errors are the “third leading cause of death.” That story is not a sober accounting of negligent medical practice. It is based on a few severely flawed studies that take the brutal uncertainty of caring for sick patients, reclassify bad outcomes as preventable deaths, and then use the resulting number to justify an ever-expanding bureaucracy.
Of course, patient safety is important. But too often, the safety narrative refuses to admit the central fact of clinical medicine: doctors are not piloting healthy passengers through a well-engineered system. We are treating human beings whose bodies are failing in complex, overlapping, and often irreversible ways.
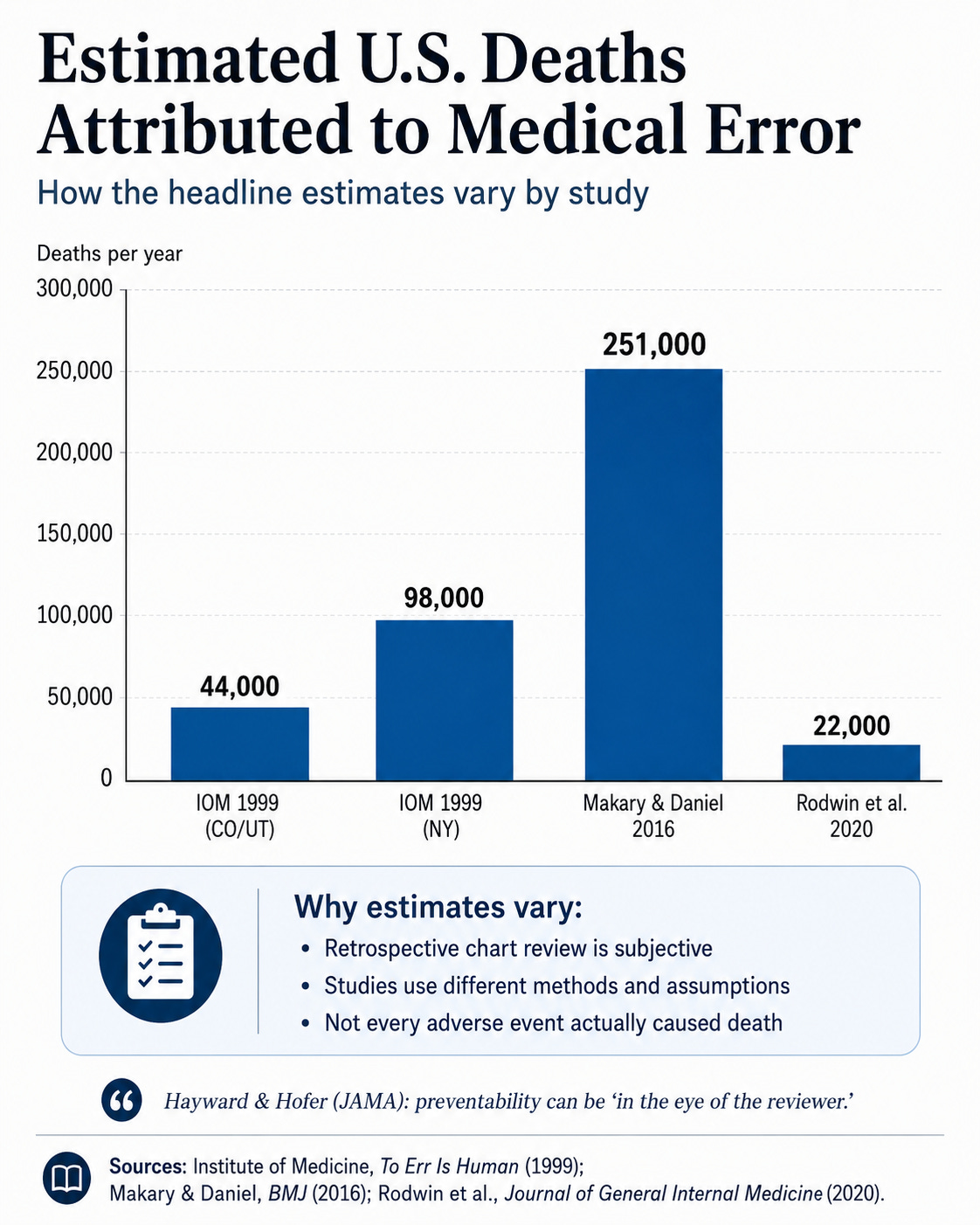
That is not a theoretical concern. In one JAMA study of hospital deaths, physician reviewers often disagreed about preventability, and the authors concluded that preventability can be “in the eye of the reviewer.” They found that while 22.7 percent of reviewed deaths were judged at least “possibly” preventable, only 6 percent were rated probably or definitely preventable. After accounting for prognosis, reliability, and the likely survival benefit of optimal care, they estimated that only about 0.5 percent of patients who died would have lived at least three months in good cognitive health if optimal care had been provided.
Yet, there is a persistent claim: that doctors are just offing patients. And it is often emphasized with the analogy that doctors are killing the equivalent of several jumbo jets full of patients every week. Then comes the inevitable appeal to aviation. If commercial pilots crashed planes at this rate, we are told, the public would revolt. Therefore, hospitals must be more like airlines.
It is a powerful analogy. It is also wrong.
Not wrong because doctors never make mistakes. We do. Every physician who has practiced long enough carries memories that do not leave. Medicine is practiced by human beings, on human beings, under uncertainty, and the stakes are often unforgiving.
But taking care of patients is not the same as flying an airplane. Every patient eventually dies. Thankfully, not every Boeing ends up in a fiery wreck strewn about fields, mountains, or oceans. Pilots generally fly an airplane only after it has been maintained and cleared. Physicians often enter the care of a patient when they are already near death, as if a pilot took over the plane as it was on fire and heading toward a mountain.
Much of medicine consists of choosing between competing dangers while knowing that either choice may end badly. Crash the plane into the forest or into the ocean. Either way, it’s going down. This is the trap hidden inside many medical error statistics. They treat adverse outcomes as if they were self-evidently preventable, instead of bad things that happen to sick people.
The modern version of this story traces back largely to two highly influential publications: the Institute of Medicine’s 1999 report, To Err Is Human, and a 2016 BMJ paper by Marty Makary and Michael Daniel arguing that medical error should be considered the third leading cause of death in the United States. The IOM report relied heavily on earlier chart-review studies from Colorado, Utah, and New York, then extrapolated those findings to the country as a whole. Using the Colorado and Utah data, the report estimated 44,000 deaths per year from medical errors; using the New York data, the estimate rose as high as 98,000. Makary and Daniel later popularized a much larger figure, more than 250,000 deaths annually.
These numbers entered public discourse as if they were direct measurements. They were not. The IOM estimates were extrapolations from state-level retrospective chart reviews. The Makary estimate was built by combining prior studies that used different methods, without a formal meta-analysis and without fully accounting for statistical uncertainty. AHRQ’s patient safety review notes that determining preventability is difficult, that physician reviewers often show only moderate agreement, and that the Makary estimate extrapolated from studies using different methodologies.
That is the first problem: the numbers sound precise, but the underlying judgment is often subjective.
The second problem is even more important. The underlying studies often struggled to determine whether an adverse event actually caused the death. Shojania and Dixon-Woods, writing in BMJ Quality & Safety, criticized the “third leading cause” claim for exactly this reason. They argued that the estimate combined prior studies too simplistically, failed to follow accepted standards for quantitative synthesis, and did not adequately address whether the adverse events detected by review tools actually contributed to death. Critically ill patients have more interventions, more adverse events, and higher mortality. That does not mean the adverse event killed them. It may mean that while an error occurred, it did not meaningfully change the outcome. Again, to the airline analogy, it’s as if a pilot gets judged for hitting a little turbulence in a plane that’s destined to crash anyway.
This is not an abstract statistical quibble. It is the difference between a patient who dies because a doctor gave the wrong drug and a patient who dies because she had metastatic cancer, septic shock, renal failure, delirium, and then experienced an adverse event during the last days of life. They are not morally or clinically the same thing.
More recent evidence suggests the older headline estimates were too high. A 2020 systematic review and meta-analysis in the Journal of General Internal Medicine estimated that about 3.1 percent of hospital deaths were preventable. Applied to the United States, that corresponded to roughly 22,000 preventable deaths per year, and about 7,000 among patients with a life expectancy greater than three months. That is still a serious number. It is not nothing. But it is not the third leading cause of death in America. It’s not even close.
The difference matters because the patients in these studies are not randomly selected healthy Americans walking around in perfect condition until a doctor harms them. They are hospitalized patients, often elderly, frail, chronically ill, acutely decompensating, or already near death. Many are receiving multiple interventions precisely because their baseline risk is high. That does not excuse preventable harm. But a bad outcome in such a patient is not automatically evidence of an error.
The public is uncomfortable with this because the public wants medicine to be deterministic. They want to prevent the next error with a new rule.
There is a tragic irony here. The exaggeration of preventable error can make genuine patient safety worse. When every adverse event becomes evidence of system failure, physicians learn to avoid risk, and systems learn to game the metrics to obscure the actual truth.
That may protect the institution. It does not necessarily help the patient.
After To Err Is Human, American medicine embraced a vast quality and safety apparatus. Some of it was valuable. Surgical time-outs, central line infection prevention, standardized handoffs, and checklists for high-risk recurring tasks can reduce harm. Pronovost’s central-line work, for example, produced large reductions in catheter-related bloodstream infections, and the WHO surgical checklist study found lower complication and death rates after checklist implementation. No serious critic should deny that safety systems can work when they target concrete, recurring, preventable failures.
But now the checklist has ballooned into a bureaucratic obstruction to actual patient care. In some hospitals, it has expanded into a lengthy ritual, including everything in the checklist from team introductions to acknowledgment of the patient’s pronouns (this is true, not hyperbole).
The problem is that the safety movement did not stop at identifying clear, preventable failures. It became a governing philosophy. It gave administrators, regulators, payers, and quality officers a moral language for controlling the clinical encounter.
From that point forward, more and more of medicine became subject to measurement from above. Physicians were asked to satisfy more and more quality metrics. As the saying goes, “not everything that counts can be counted, and not everything that can be counted counts.”
This burden is not theoretical. A Health Affairs study by Lawrence Casalino and colleagues estimated that physician practices in four common specialties spent an average of 785 hours per physician per year dealing with quality measure reporting, at a cost of more than $15.4 billion annually. That is time, labor, and attention pulled away from actual patient care and redirected toward measurement infrastructure.
Hospitals face the same machinery on a larger scale. A JAMA study found that Johns Hopkins Hospital was reporting 162 quality metrics across multiple programs. The authors estimated that collecting and reporting those metrics required 108,478 person-hours and more than $5 million in personnel costs, plus more than $600,000 in vendor fees, in a single year. Extrapolated across thousands of acute care hospitals, the authors suggested the national burden runs into the billions.
Private practices feel this even more acutely. A small independent physician group does not have an army of compliance officers. It has doctors, nurses, medical assistants, and maybe a thin administrative staff trying to keep the doors open. Every new reporting requirement adds fixed cost. Large hospital systems can absorb those costs, spread them across departments, and then use compliance complexity as another reason independent physicians should sell. This is one way the quality-metric industrial complex becomes another force driving consolidation.
That consolidation is not hypothetical. The AMA’s 2024 physician practice benchmark found that only 42.2 percent of physicians were working in private practice, down from 60.1 percent in 2012. Over the same period, the share of physicians working for hospital-owned practices or directly employed by hospitals increased. Regulation does not always harm the largest incumbents. Often, it protects them by raising the fixed cost of survival.
This is one of the recurring patterns in American health care. A problem is identified, often a real one. A centralized solution is proposed. The solution requires measurement, reporting, enforcement, and administrative infrastructure. Large organizations adapt. Small organizations struggle. The burden then becomes an argument for more consolidation, more standardization, and more bureaucracy. Eventually, the original problem remains, but now we have fewer independent physicians, higher costs, and more people whose jobs depend on the machinery continuing to expand.
And once the metric becomes the target, the system starts optimizing for the metric.
Anyone who has worked in hospitals has seen versions of this. Patients are transferred between services in ways that make the mortality numbers look better for one department and worse for another. Documentation specialists hound doctors to capture every comorbidity so the patient appears as sick as possible on admission, which improves risk-adjusted performance. Hospitals test urine on admission, in part because if an infection is coded as “present on admission,” it is quantified differently than if it is coded as hospital-acquired. CMS policy explicitly distinguishes conditions present on admission from selected hospital-acquired conditions, and hospitals can face payment consequences for certain conditions not present on admission.
In some cases, the metrics actually cause more deaths. This happened when the readmission reduction program successfully reduced the number of heart failure patients being readmitted to the hospital. Unfortunately, as readmissions dropped, mortality rose. Patients who needed readmission were sent home, rather than bring down the hospital’s statistics. They died because of a metric.
The more we attach money, reputation, and punishment to simplified metrics, the more sophisticated institutions become at managing the numerator, the denominator, and the documentation surrounding both.
These are all byproducts of a system that rewards metrics more than patient care because people thought the metrics could fix patient care.
They cannot.
Bad things happen to sick people. That sentence sounds harsh only because modern health care has trained us to speak as if mortality itself were a quality defect. But every physician knows it is true. The doctor is not the only causal force in the room.
The medical error narrative, as commonly presented, offers the public a fantasy that enough regulation can make illness behave like a mechanical system. It tells policymakers that if doctors would simply comply with more rules, hundreds of thousands of deaths might disappear.
The honest path is harder. It begins by admitting that medical care involves tradeoffs, not guarantees.
Doctors should be accountable. But accountability built on inflated statistics and bad analogies will not make patients safer. It is doing the opposite, replacing judgment with metric gaming.
Doctors are not crashing jumbo jets. They are caring for fragile human beings in a world where risk cannot be abolished, only moved around. The sooner we admit that, the sooner we can have a serious conversation about patient safety.
The anticoagulation case is doing more work than the aviation analogy, because it shows how hindsight changes the moral shape of a decision. Before the outcome, the clinician is choosing between two dangers. After the outcome, only one danger has a body attached to it, and the other becomes a cleaner counterfactual.
That asymmetry is what makes retrospective judgment so treacherous. If the hemorrhage expands, continuing the anticoagulant looks reckless; if the stroke comes, reversing it looks reckless. The choice itself never became simple. The bad outcome merely gave one side of the dilemma a witness.
Accountability still matters here, and if anything it has to be more exacting. The serious question is not whether harm occurred, but whether the decision respected the risk landscape that existed before anyone knew which harm would become real. Patient safety is undermined when it lets hindsight pretend the uncertainty was never there.
Should this be framed as the detecting fault in doctors or fault in hospitals?
My admittedly personal and anecdotal experience suggests to me that hospitals are dangerous places. And, not because of what doctors are doing. You make good points about the inevitable dilemmas in choosing strategies for treatment and care. My personal experience and anecdotal examples suggest that the casualty count is being run up well outside the scope of such dilemmas. That’s what makes the jumbo jet numbers plausible to me.
Hospital-acquired infections are just one category associated with jumbo jet numbers.