
A Safety Net or a Slush Fund?
Medicaid, Waivers, and the Price of Pretending Everything Is Health Care
I’m seeing a Medi-Cal patient in my neurosurgery clinic in California. He has low back pain from a herniated disc compressing a nerve root. In many cases, an epidural steroid injection can quiet the inflammation, reduce the pain, and buy enough time for the disc herniation to improve without surgery.
But in California, getting that injection for a Medi-Cal patient can mean a wait measured in months. In my world, a six-month wait is not unusual.
Part of this is a payment-and-capacity problem. This is not some exotic operation. It is ordinary pain medicine. Yet for my patient, who is sitting in front of me in real pain, the system cannot reliably provide it in a timely fashion.
And yet California’s Medicaid program can find a way to pay for “Traditional Healers” and “Natural Helpers.”
The official language is more sanitized than that. California’s Medi-Cal program, through its CalAIM waiver structure, now covers “traditional health care practices” for certain Medi-Cal and CHIP beneficiaries. DHCS says Traditional Healer services may include traditional music, songs, dancing, drumming, ceremonies, rituals, herbal remedies, and spirituality. The state also says it does not require Traditional Healers or Natural Helpers to have a separate state license or certification.
That fact alone is jarring enough. But the deeper issue is not merely that California has decided to pay for spiritual or quasi-spiritual services through Medicaid. The deeper issue is that this example opens a window into how Medicaid financing actually works. It shows how a program that most ordinary people imagine as health insurance for the poor has become a complicated fiscal machine, one that mixes state money, federal money, hospital taxes, local transfers, managed-care contractors, waiver authority, and political discretion. By the time the money comes out the other end, almost no one can tell who is really paying, who is really benefiting, and what care is being crowded out.
The point is not that every Traditional Healer is committing fraud. That would be the wrong claim, and it would be unfair. Cultural support is not fraud just because it is not Western medicine. The point is narrower and more important: Medicaid has built a financing architecture in which the most concrete medical services often face the hardest prospective review and the worst funding, while some of the hardest-to-verify services are policed mainly through retrospective oversight. That is the kind of architecture that makes fraud easier in hospice, home health, autism therapy, and other services where the payer cannot easily see what actually happened. We see this in national headlines today.
To understand how California can pay for something like this, you need to understand four pieces of Medicaid financing. First, Medicaid is jointly funded by states and the federal government through matching funds. Second, much of Medicaid is now run through managed-care plans that receive a monthly payment per enrollee. Third, states can use waivers to pay for things ordinary Medicaid rules might not otherwise cover. Fourth, states can use provider taxes, local transfers, supplemental payments, and state-directed payments to make the true source and destination of Medicaid dollars almost impossible for a normal person to follow.
Medicaid Is Not One Checkbook
Most Americans understand Medicare a little more easily than Medicaid. Medicare is a federal program, mostly for the elderly and disabled. Medicaid is different. Medicaid is jointly financed by the federal government and the states. Every state runs its own program within broad federal rules, and the federal government matches state Medicaid spending according to a formula called the Federal Medical Assistance Percentage, or FMAP.
KFF’s Medicaid financing overview explains the basic structure well. Medicaid is administered by states within broad federal rules and jointly funded by states and the federal government through a federal matching program with no preset cap. Poorer states generally receive a higher match. Wealthier states receive less. The statutory floor for the traditional Medicaid match is 50 percent, meaning the federal government pays at least half of ordinary Medicaid benefit costs.
Traditionally, Medicaid covered certain categories of low-income people: poor children, poor pregnant women, low-income parents, the disabled, and poor elderly patients needing long-term care. The Affordable Care Act expanded Medicaid to cover low-income able-bodied adults, and for that expansion population the federal government pays 90 percent of the bill. In federal fiscal year 2024, total Medicaid spending was about $919 billion, with the federal government paying roughly $594 billion and states paying about $325 billion.
This is the first thing to understand: Medicaid is built around matching funds. If a state spends an eligible Medicaid dollar, Washington sends money back. If the match rate is 50 percent, the state puts up 50 cents and the federal government puts up 50 cents. If the match rate is 90 percent, the state puts up 10 cents and the federal government puts up 90 cents.
That matching structure changes the politics of spending. If Sacramento spends a purely state dollar on something, California taxpayers bear the full cost. But if Sacramento can define that same expenditure as Medicaid spending, it may pull in federal matching dollars. That does not make the spending free. It just moves part of the bill to federal taxpayers. It also creates a strong incentive for states to expand the category of what counts as Medicaid and for whom that coverage is offered.
How Medicaid Pays for Care
The simplest version of Medicaid is fee-for-service. A patient sees a doctor, receives a service, and the state Medicaid program pays a fee for that service. An office visit has one rate. A CT scan has another rate. A hospital stay has another. This is the easiest model to understand because it resembles a direct transaction, although with the government standing between the patient and the clinician.
If a doctor visit costs $50 and the patient is part of the ACA Medicaid expansion group, the state may pay only $5 while the federal government pays $45. If the patient is in a traditional eligibility group in a state with a 50 percent match, the state pays $25 and the federal government pays $25.
Fee-for-service has obvious problems. If the state pays every time a service is delivered, there is an incentive to deliver more services and more intense services. A state can still impose utilization management. But the basic payment logic is transactional: a covered service is billed, documented, and paid.
That model is especially vulnerable when the service is hard to verify after the fact. It is one thing to confirm that an MRI was performed. It is another to confirm whether a home health visit happened for the hours billed, whether a hospice patient was truly eligible, whether an autism therapy session was one-on-one or group care, or whether a traditional healing encounter delivered what the claim form says it delivered.
So states moved heavily into managed care. Instead of paying each doctor and hospital directly for each individual service, the state contracts with a managed care organization, or MCO, and pays that plan a fixed amount per member per month. This is called a capitated payment. The managed-care organization then administers the insurance benefit. It builds networks, negotiates with providers, manages utilization, and takes financial risk. If the plan spends less than the capitation payment while meeting its contractual obligations, it can keep the difference. If it spends more, it loses money.
Different states choose MCOs in different ways. Some use competitive procurement, where plans respond to a request for proposals and the state selects plans based on network adequacy, quality, administrative capacity, cost, and other factors. Some states or counties have multiple plans from which patients can choose. Others have only one dominant public or quasi-public plan. California has a complicated hybrid structure, with county organized health systems in some counties, two-plan models in others, and more competitive plan environments in places like Sacramento and San Diego.
Because managed care gives states more budget predictability and delegates utilization management to plans, states have shifted much of Medicaid into MCOs. KFF reports that capitated payments to comprehensive Medicaid managed-care organizations accounted for about half of Medicaid spending in federal fiscal year 2024.
The law requires these managed-care rates to be “actuarially sound.” In plain English, that means the state cannot just make up a number. The payment rate has to be developed according to actuarial standards and be adequate to cover the reasonable, appropriate, and attainable costs of providing covered Medicaid services to the enrolled population under the contract. Federal regulations require CMS review and approval of those rates.
Actuarial soundness does not mean a Medicaid plan won an open auction to treat patients for the lowest price. It means the state, its actuaries, the managed-care plan, and CMS agree that the per-member-per-month payment is projected to cover the cost of covered services for that population. The state may use competitive procurement, require network and quality demonstrations, and select one or more plans by county. But the rate still has to fit within a CMS-approved actuarial framework.
Confused yet? It gets more confusing.
Federal rules say what Medicaid must cover. Whether under fee-for-service or managed care, Medicaid has mandatory benefits and optional benefits. Physician services, hospital services, nursing facility care, laboratory services, and many other core services fall within the traditional medical benefit structure. But as you can probably guess, “faith healers” are not on the ordinary list of mandatory Medicaid benefits.
So how does something like that get covered? How does a state decide to cover something extra and still get the federal government to pick up part of the bill?
The Waiver: How Exceptions Become Policy
Now we get to the machinery that allows Medicaid to pay for things most people would not intuitively think of as medical care.
Section 1115 of the Social Security Act gives the federal government authority to approve experimental, pilot, or demonstration projects that are likely to promote the objectives of Medicaid. CMS says these demonstrations must be budget neutral to the federal government, meaning federal Medicaid spending under the waiver should not exceed what federal spending would have been without it. Federal guidance also explains that Section 1115 can authorize federal matching funds for state expenditures that would not otherwise be eligible for federal Medicaid reimbursement.
That last sentence is the key. A waiver can take something that ordinary Medicaid rules might not pay for and turn it into matchable Medicaid spending.
California’s CalAIM waiver is one of these demonstrations. CMS approved California’s Traditional Health Care Practices amendment in October 2024. Once approved, the state could treat certain traditional healing services as Medicaid expenditures and claim federal matching funds under the terms of the demonstration.
The theory is simple. California comes to CMS and says that these services will help Medicaid beneficiaries. The state submits projections suggesting that the program will remain budget neutral because the new spending will be offset by reduced spending elsewhere or by other assumptions embedded in the waiver model. CMS reviews the proposal and approves the demonstration if it decides the waiver promotes Medicaid’s objectives and satisfies federal requirements.
But the counterfactual is modeled, not proven. Budget neutrality is built against a hypothetical without-waiver baseline. That may satisfy a federal budget office, but it does not prove that the new service actually improved care or saved money in the world where patients live.
This was supposed to be a tool for experimentation. In theory, states could test whether a new way of delivering care improves outcomes and saves money. That is not inherently bad. Medicaid is a huge program. The country is diverse. States differ. A rigid national rulebook will not always make sense.
But the same flexibility can also become a loophole. Once the door opens to “demonstrations,” the definition of health care can expand. Housing supports, Uber rides, and food vouchers all become health care. Some of these programs may be humane. Some may even be useful. But every expansion changes Medicaid from a safety-net medical program into a general social-policy financing vehicle.
It also lets states direct money toward favored priorities while the federal government picks up much of the tab. If the spending is tied to the ACA expansion population, the federal government can pick up 90 percent. The state is responsible for fiscal discipline, but the federal government is paying most of the bill.
What Exactly Is California Paying For?
The state’s own documents are worth reading because they show how elastic the language has become.
California says Traditional Healer services may include practices such as music, songs, dancing, drumming, ceremonies, rituals, herbal remedies, and other forms of spirituality. Natural Helper services may include community navigation, psychosocial support, trauma support, wellness support, and assistance with self-management and recovery. The state says these services are part of substance use disorder treatment for eligible beneficiaries in participating counties and facilities. DHCS says it does not require Traditional Healers or Natural Helpers to hold a state license or certification.
There are also documentation and claiming rules. Participating providers must submit opt-in packages. Counties and DHCS have roles in approval, claims processing, and monitoring. Claims must be submitted through Drug Medi-Cal Organized Delivery System counties. So it would be inaccurate to say there is literally no oversight.
But what the state does not do is the very thing it often does to physicians: require an outside reviewer to decide whether this service is clinically necessary for this patient before payment. In fact, DHCS says neither DHCS nor DMC-ODS counties may determine whether a traditional health care practice is culturally or clinically appropriate for an individual Medi-Cal member. That decision is made by the Traditional Healer or Natural Helper.
That is the asymmetry.
A neurosurgeon trying to get an MRI or an injection for a patient with neurologic symptoms may have to justify the request to a distant reviewer using documentation, guidelines, imaging criteria, and clinical evidence. But for these traditional practices, the state is far more deferential. The clinical appropriateness decision is not made by the payer. It is made within the very structure being paid.
The payment rates are not symbolic either. For state fiscal year 2025–2026, DHCS lists an all-inclusive rate of $801 for eligible Traditional Healer and Natural Helper services in certain settings. For services not eligible for the all-inclusive rate, DHCS lists $801 for Traditional Healer services and $335.37 for Natural Helper services.
A reasonable person can support culturally respectful care while still asking a very basic question: why is Medicaid, a program that routinely struggles to provide timely access to physicians, imaging, surgery, psychiatry, and addiction treatment, paying hundreds of dollars per encounter for services that include ceremonies, rituals, drumming, and spirituality?
Where Opacity Becomes Fraud Risk
This is where the argument must be careful.
The Traditional Healer benefit is not fraud. Fraud is a crime. Cultural support is not fraud just because it is not Western medicine. A ceremony is not a false claim merely because a physician would not prescribe it.
The point is not that Traditional Healers are fraudsters. The point is that Medicaid becomes vulnerable when it pays for services that are difficult for an outsider to verify, delivered outside ordinary clinical settings, billed by encounter or time, and policed mainly through documentation after the fact.
That pattern keeps showing up in the parts of government health care that produce scandals.
Hospice fraud often turns on whether a patient was truly terminal, whether the patient even knew he was enrolled in hospice, and whether services were actually provided. California officials recently charged 21 people in an alleged $267 million Medi-Cal hospice fraud scheme involving stolen identities, 14 hospice companies, and billing for services tied to people who allegedly had no idea their identities had been used.
Home health fraud often turns on whether an aide actually showed up, for how many hours, and whether the patient truly needed the service. In 2026, Reuters reported that CMS imposed a six-month nationwide moratorium on new Medicare enrollments for home health and hospice providers, citing fraud concerns. The policy itself may or may not be well designed, but the reason for it is revealing: these are services where billing can outrun verification.
Autism therapy has become a similar warning sign. The Wall Street Journal reported that Indiana barred Piece by Piece Autism Centers from Medicaid after the company received about $340,000 per patient on average in 2023. In Connecticut, local reporting described an autism-related Medicaid fraud case involving thousands of allegedly false behavioral therapy claims for services that were not performed or not properly supervised. These cases differ in their details, but the vulnerability is similar: when a payer is billed for hours, encounters, supervision, and subjective services it cannot easily observe, the system becomes much easier to game.
Even the official improper payment data should be understood with care. Improper payments are not the same thing as fraud. KFF notes that improper payments are often the result of missing documentation, insufficient information, or failure to follow administrative requirements rather than proof that the patient, provider, or service was illegitimate. CMS’s 2025 Medicaid improper payment data estimated a national rolling Medicaid improper payment rate of about 6 percent.
But improper payments still matter because they reveal the basic administrative problem. The government is trying to run a massive program with billions of claims, millions of enrollees, thousands of provider types, multiple financing streams, and services that range from a complex brain surgery to a home health visit to an autism therapy session to a spiritual healing encounter. Some of those services are easy to verify. Many are not.
This is why the faith-healer example is so useful. It makes the verification problem visible. If Medicaid pays for an MRI, we can generally confirm that an MRI occurred. If Medicaid pays for surgery, there is an operative note, anesthesia record, implant log, hospital bill, and recovery course. These systems are imperfect, but the service is concrete.
But if Medicaid pays for a traditional healing encounter that may include music, drumming, ceremony, herbal remedies, spirituality, or psychosocial support, what exactly is the outside reviewer verifying? That a claim form was submitted? That a note was written? That the provider said the encounter occurred? That the participating organization deemed the practitioner qualified? That the service was culturally appropriate according to the very people delivering it?
That is not the same type of oversight physicians face when they request conventional care.
Again, that does not prove fraud. It proves that the ordinary tools of medical verification are weaker. And when the tools of verification are weak, the system becomes easier for bad actors to exploit.
So back to my patient with the herniated disc. He is covered under managed care, so there is a layer of utilization review. To be clear, I do not object to utilization management in principle. I do not believe insurance companies or taxpayers should pay for a service simply because a doctor says so. Public money should be scrutinized. Some utilization management is necessary.
But the system applies skepticism unevenly.
When a physician requests a steroid injection the system demands documentation, medical necessity, guidelines, and often prior authorization. But when a service is politically protected, culturally framed, waiver-approved, and difficult to verify, the same system can become remarkably deferential.
The Federal Match Game
To understand why states pursue arrangements like this, one must return to the match.
Suppose California spends $10 million on a state-only program. California pays $10 million. But suppose California can place that program inside Medicaid and claim a 50 percent federal match. Now California pays $5 million and the federal government pays $5 million. If the match is 90 percent, California pays $1 million and the federal government pays $9 million.
That is why Medicaid waivers are so attractive. They transform the political economy of spending. A state program that would be expensive with state-only dollars becomes easier to justify when federal taxpayers pick up a large share of the bill.
But money does not become free because the bill is divided between governments. Federal taxpayers are still taxpayers and Medicaid administrative capacity is still finite.
The deeper problem is that matching funds weaken fiscal discipline. When a state buys something with its own money, voters can at least see the tradeoff more clearly. When a state buys something with Medicaid matching funds, the price is disguised. The state can say, in effect, “we only paid 10%.” But the country paid the whole thing.
California is a useful case study because Medi-Cal has become enormous. The program covers roughly 15 million people (double from 2010 levels), and per-enrollee spending has grown 5.4% year-over-year, outpacing inflation. In 2026, California officials were dealing with a multibillion-dollar Medi-Cal financing gap, with the state borrowing $3.44 billion and requesting another $2.8 billion to cover program costs, according to Associated Press reporting. That is the strange reality of modern Medicaid: the program can be huge, expensive, and still unable to reliably provide timely access to ordinary care.
Provider Taxes, Local Transfers, and the Art of Making the State Share Appear
The financing gets even stranger because states do not always fund their Medicaid share through ordinary state tax revenue. They can use provider taxes, intergovernmental transfers, and certified public expenditures.
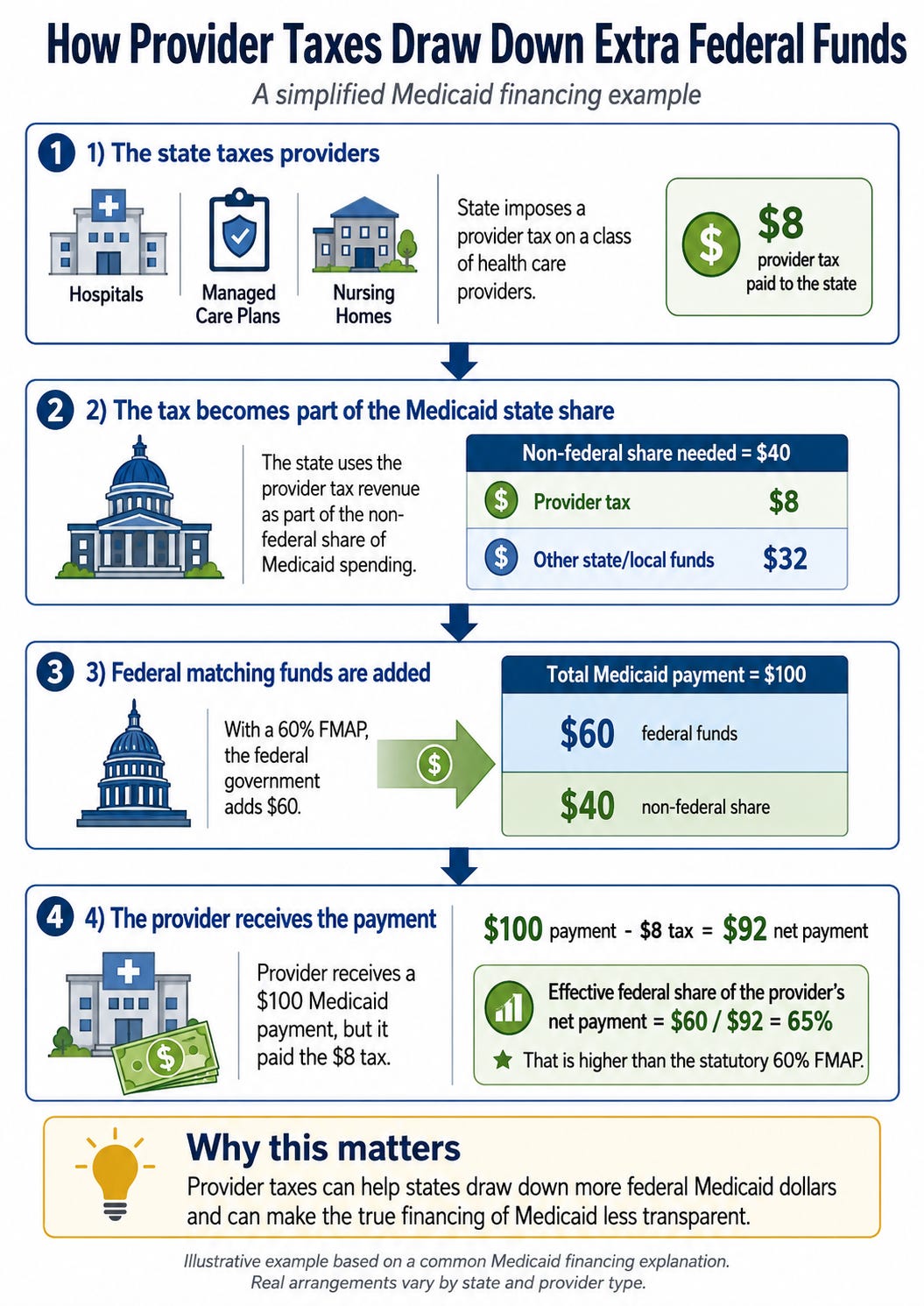
A provider tax is exactly what it sounds like. The state taxes a class of health care providers, such as hospitals, managed-care organizations, or nursing facilities, and uses the revenue as part of the non-federal share of Medicaid spending. Because those taxes are considered non-federal spending, that spending then draws down federal matching funds. Often, the same provider class that pays the tax receives increased Medicaid payments.
This is legal within federal limits, but the fiscal effect can be very different from what the public imagines. KFF explains that states use provider taxes, intergovernmental transfers, and certified public expenditures to help finance the non-federal share of Medicaid. MACPAC has explained that provider-financed payments can make the effective federal share higher than the statutory FMAP. In one example, if a state has a 60 percent FMAP and a provider pays an $8 tax that helps finance a $100 Medicaid payment, the federal government still contributes $60, while the provider nets $92 after tax. The effective federal share of the net payment becomes about 65 percent rather than 60 percent.
An intergovernmental transfer, or IGT, is a transfer of public funds from a local government entity to the state Medicaid agency. A county hospital, public hospital district, or local government can transfer money to the state. The state uses that money as the non-federal share and claims federal matching dollars.
Certified public expenditures, or CPEs, work differently. A public entity certifies that it has spent money on Medicaid-eligible services, and the state uses that certified spending to claim federal matching funds.
In plain English, states have learned how to turn provider and local-government money into federal Medicaid money.
Some of this supports real care. Some of it keeps safety-net hospitals alive. Some of it raises Medicaid payments closer to Medicare or commercial rates, which can improve access if designed properly. But the mechanism also makes Medicaid less transparent. A voter hears that the state is spending more on Medicaid. A hospital says it is being taxed. A federal agency says it is matching state expenditures. A managed-care plan says it is passing through state-directed payments.
This is not simply Medicaid paying doctors for poor patients. This is Medicaid as fiscal engineering. A provider tax can become the state share. The state share can become federal matching funds. The matching funds can become higher payments. The higher payments can move through managed-care plans as state-directed payments. Each piece can be legally defensible. Together, they make the program almost impossible for voters to audit.
State-Directed Payments: The Managed-Care Back Door
There is one more piece of the machinery that matters: state-directed payments.
Remember, in managed care, the state pays an MCO a monthly capitation payment, and the MCO pays doctors, hospitals, and other providers. In theory, this means the plan is managing cost and utilization. But states can also direct managed-care plans to make specific payments to providers.
Sometimes this can be used to support rural providers and keep a facility’s doors open when patient volume is low. Sometimes it can help bring Medicaid reimbursement closer to Medicare or commercial rates for services where there are shortages. Sometimes it can help safety-net providers survive. And sometimes it can route enormous sums to politically connected hospital systems that have learned to cry poor while expanding their market power.
CMS explains that federal Medicaid managed-care rules allow states to direct certain payments by managed-care plans to providers. MACPAC describes these arrangements as including minimum fee schedules, value-based payments, and uniform rate increases. Some states have used them to make large additional payments to providers in ways that resemble supplemental payments in fee-for-service Medicaid.
The scale is enormous. MACPAC reported that between February 2023 and August 2024, CMS approved 302 distinct directed-payment arrangements in 40 states and Puerto Rico, with projected spending of $110.2 billion per year. Many of the largest arrangements were directed to hospitals and financed through provider taxes or intergovernmental transfers. MACPAC also noted that rigorous evaluations are limited and that provider-level data gaps make it hard to assess whether these payments actually achieve their stated goals.
This matters because it shows how far Medicaid has moved from the simple idea of paying for care for poor patients. The modern program is a web of capitation payments, supplemental payments, directed payments, waiver expenditures, provider taxes, local transfers, and federal matching claims.
Some of these mechanisms may be necessary in a badly distorted system. But taken together, they create a program in which the loudest and most politically organized actors often do better than the quietest and sickest patients.
The Zero-Sum Reality
Defenders of expansive Medicaid waivers often reject the idea that there is a tradeoff. They will say the Traditional Healer benefit is small relative to the Medicaid budget. They will say it is targeted. They will say it is culturally appropriate. They will say it does not directly take away an MRI from a patient with back pain.
Some of that may be technically true in the narrow accounting sense. Medicaid is not a coffee can filled with dollar bills where one person’s drumming ceremony directly removes another person’s epidural steroid injection. The financing is more complicated than that.
California and CMS were able to build a pathway to pay for Traditional Healers and Natural Helpers. They were able to define the benefit, identify eligible settings, authorize federal matching funds, establish payment methodologies, describe documentation rules, and clarify claiming procedures. The state can figure out how to reimburse ceremonies, rituals, drumming, herbal remedies, and spirituality through Medicaid.
Yet patients are still waiting 6 months for a legitimate medical procedure which should take 6 days to arrange.
A safety-net program must make choices. It cannot fund everything. It cannot be health insurance, housing policy, food policy, income support, cultural restoration, spiritual counseling, addiction treatment, hospital subsidy, managed-care profit center, and general-purpose federal matching strategy all at once without losing sight of its central purpose.
Coverage is not the same as care. A Medicaid card does not decompress a spinal cord. The inputs that matter in medicine are stubbornly concrete. Physician time and capacity is scarce. Pretending otherwise does not make us compassionate. It makes us unserious.
A Safety Net Needs a Floor, Not a Slush Fund
Medicaid was created for a moral purpose. It was supposed to provide medical care to people who could not otherwise afford it. That mission is worth defending.
But precisely because the safety net matters, it must be disciplined. Scarcity is not cruelty. Scarcity is the reason discipline is necessary. If we pretend Medicaid can be everything, the people with the least power will be the first to discover that it is not very good at being anything.
A serious Medicaid program would start with a floor. It would guarantee access to essential, evidence-based medical care. It would pay enough to maintain real physician networks. It would reduce administrative friction for high-value care. It would measure success by whether patients can actually see doctors, obtain imaging, receive treatment, and recover function. It would treat the time of physicians, nurses, and patients as valuable and reward them for taking on these challenging patients. It would stop confusing coverage expansions with care delivery.
Instead, we have built a system that often underpays real clinicians, overpays intermediaries, subsidizes consolidated hospital systems, creates an architecture in which fraud is easier to hide, hides prices, taxes providers to draw down federal funds, and then congratulates itself for funding “innovation.”
Now that same system can pay for Traditional Healers while patients wait for ordinary medicine.
When a state can find the administrative will to reimburse rituals but cannot reliably get a patient timely specialty care, the problem is not a lack of money alone. It is a collapse of priorities.
And in Medicaid, as in all of health care, the people who pay the highest price for collapsed priorities are usually the patients with the fewest choices.